Homeopathy treats underlying cause of anemia. Diagnosing cause of anemia and select medicine accordingly helps many anemic patients. In iron deficiency anemia homeopathic medicines are very effective. Dietary deficiency should be correct. The digestive and assimilative capacity or an inability to absorb iron can be corrected. Treatment on individualized bases helps body to absorb nutrients from food naturally.
Homeopathic medicines for anemia
There are many medicines for anemia, which medicine is best for you is only prescribed after complete case taking. Following are the homeopathic medicines for anemia
China (Cinchona), Calcarea ars, Ferrum phos, Ferrum metallicum, Ferrum pic, Ferrum aceticum, Helonias dioica, Kali carb, Lecithinum, Natrum mur, Pulsatilla Arsenic Iridium met, Acid phos, Graphites, Trifolium pretense, Aletris farinose, Crotalus horridus, Alumina, Abrotanum, Sepia officinalis and many others
Anemia
Not sufficient red blood cell / erythrocyte to carry oxygen to tissues is a condition known as anaemia. There are many causes of anaemia. It can be for short time or long time, acute anameia because of injury or acute hemorrhage and chronic anaemia in patients with long-standing diseases or illness. In Pakistan anaemia is common among women and also in children, 37 percent among pregnant and 26 percent among non-pregnant women.
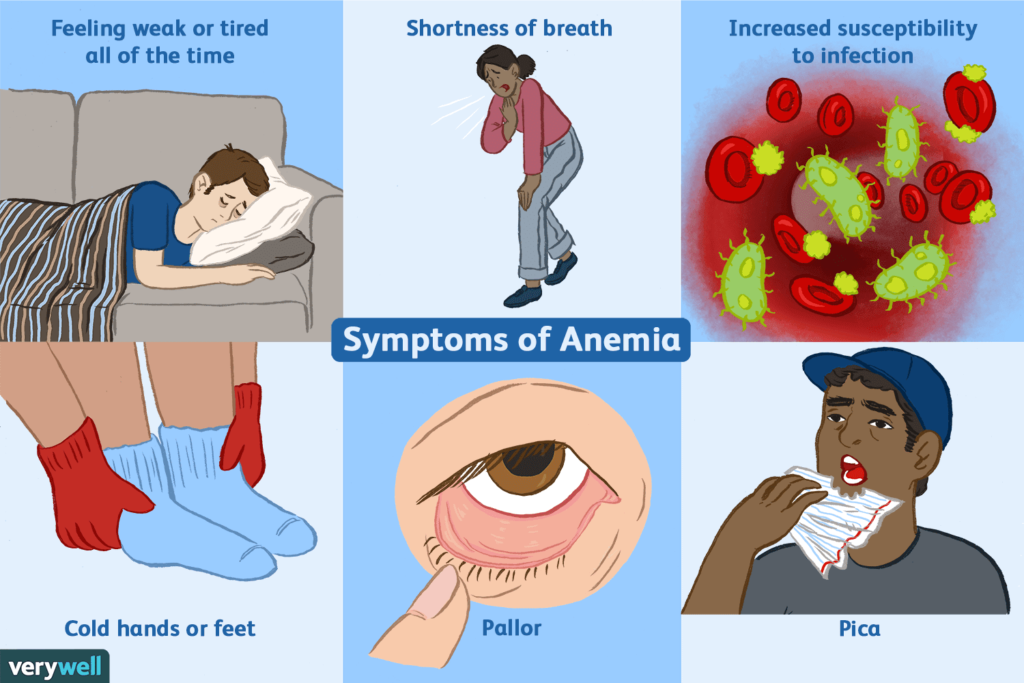
Symptoms of anemia includes :
• Weakness
• Low energy
• Dizziness
• shortness of breath;
• palpitations
• pale appearance
Symptoms of severe anemia may include:
• chest pain, angina
• fainting
• Rapid heart rate.
In some people color of stool also change, low blood pressure and heart murmur. Anemia can be a warning sign of serious illness, complete checkup is necessary.
Types of Anemia
The types of anemia depend on the cause. Following classification of anemia based on cause:
• Iron deficiency anemia
• Megaloblastic anemia
• Hypoplastic anaemia
• Haemolytic anemia
• Normocytic anemia
Iron deficiency anemia
Normal requirement of iron in men is 1 to 2 mg and in women 3 mg. Deficient intake of iron, high requirement (as during pregnancy) or malabsorption of iron leads to this kind of anemia.
Megaloblastic anemia
Vitamin B12 and folic acid are important for erythropoiesis, deficiency of both cause immature and abnormally large red blood cell (megaloblast). In this anemia cells are fragile with reduced life span 40 to 50 days.
1) Vitamin B12 deficiency anemia
Pernicious anemia: it is an autoimmune disease in which autoantibodies destroy intrinsic factor (IF) and parietal cells in the stomach.
Other cause of vitamin B12 deficiency includes, Dietary deficiencies of vitamin B12, gastrectomy, chronic gastritis, malignant disease, ionizing radiation, malabsorption as in crohn’s disease or if terminal ileum is removed. Vitamin B12 deficiency cause irreversible neurological damage.
2) Folic acid deficiency anemia
Foods like leafy green vegetables, beans, citrus fruits, dried pulses are source of folic acid. Causes of this anemia include dietary deficiency, malabsoption (celiac disease) interference with folate metabolism.
Hypoplastic anaemia
Hypoplastic and aplastic anemia is cause by failure of bone marrow to produce blood cells is a rare and serious condition. Hematopoietic Stem cells in the bone marrow produce blood cells, erythrocyte, leukocyte, and platelets. Reduced bone marrow function is hypoplastic, no function in aplastic anemia.
Haemolytic anemia
Destruction of red blood cells because cells are abnormal or the spleen is overactive. Haemolytic anemia may be inherited/ congenital or acquired.
1) Congenital hemolytic anemia
This genetic condition cause abnormal haemoglobin synthesis, problem with cell membrane, reduced oxygen carrying capacity and life span.
Sickle cell anemia: RBCs appear as sickle and crescent shape. Sickle cells do not move smoothly through small blood vessels which results in increase blood viscosity; reduce blood flow leads to intravascular clotting, ischemia and infarction.
Thalassaemia: inherited disease that affects hemoglobin because of reduced globin synthesis leading to early haemolysis.
Pyruvate Kinase Deficiency
If body does not have enough pyruvate Kinase enzyme, red blood cells break easily.
Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is error of metabolism causes red blood cells to break down prematurely. It is the most common enzyme deficiency in humans.
Hereditary Spherocytosis
In Hereditary Spherocytosis red blood cells become spheres like instead of flattened discs which reduces life span to 10 to 30 days only.
2) Acquired Hemolytic Anemias
There are several causes:
Chemical/ drugs
Chemical compounds including lead and arsenic compounds from work environment or some drugs if taken for a long time cause haemolysis.
Immune Hemolytic Anemia
When immune system mistakenly form antibodies against body’s own red blood cell and break them down. Immune hemolytic anemia are autoimmune hemolytic anemia (AIHA), alloimmune, and drug-induced. Some conditions can cause AIHA including lupus, Hepatitis, HIV, Mycoplasma pneumonia, and chronic lymphocytic leukemia
Normocytic Normochromic Anemia
Normocytic anemia is when red blood cells are normal in sized low in number. Proportion of reticulocyte may be increase as body tries to restore RBCs to normal level. It is usually a consequence of other diseases including renal disease, ulcer, chronic inflammation, sever hemorrhage, malignant disease (cancer), hypothyroidism and polymyalgia rhematica.
How to diagnose anemia? What are the tests for diagnosing anaemia?
Complete blood count (CBC)
First important test is CBC. It helps in diagnosing type of anemia and severity. Hemoglobin and hematocrit figures are used to diagnose anemia. CBC Report show characteristic changes of red blood cell
Microcytic (small red blood cell size)
Macrocytic (large red blood cell size)
Normocytic (normal red blood cell size)
Hypochromic (pale red blood cell)
Blood smear: This test is order if CBC result is not normal to find out the size, shape, number, and appearance of different type of cells.
Size
• Anisocytosis
• Macrocytosis- megaloblastic anemia
• Microcytosis: iron deficiency anemia or thalassemia.
Shape
Following are the abnormalities found in RBC shape
• Echinocytes
• Elliptocytes, RBCs oval in shape- ovalocyte
• Acanthrocytes
• Fragmented cells (Schistocytes, Keratocyte, Helmet cell
• Rouleaux
• Target cells (leptocytes or codocytes)
• Sickle cells
• Teardrop cells (dacrocytes): seen in people with myelofibrosis and thalassemia.
• Spherocytosis: present inhereditary spherocytosis or due to an immune hemolytic anemia.
• Poikilocytosis
Color
• Hypochromasia means RBC are pale in color due to insufficient hemoglobin found in thalassemia and iron deficiency.
• Hyperchromasia: increased color intensity or RBCs are darker in color found in dehydration
• Polychromasia: (poly (many), (chromasia)-color.) blue-staining RBCs show the presence of immature cells
Abnormal structures within the red blood cell
• Nucleated RBCs (NRBCs) are immature RBCs found in fibrosis or tumor; may be seen in severe anemia, myelofibrosis, in chronic low blood oxygen, thalassemia, cancers that involve the bone marrow
• Heinz bodies: enzyme (G6PD) deficiency, thalassemia, and autoimmune hemolytic anemia.
• Howell-Jolly bodies- found in people with sickle cell anemia, hemolytic anemia or megaloblastic anemia, and in patient with splenectomy
• Reticulocytes: Increased numbers of reticulocytes seen with glucose-6-phosphate dehydrogenase (G6PD) deficiency, acute blood loss, RBC destruction and in other conditions
• Siderocyte, sideroblast, ring sideroblast
• Basophilic stippling is found in heavy metal poisoning, nutritional deficiencies, or myelofibrosis.
• Cabot’s Rings
Stool hemoglobin test:
Fecal Occult Blood Test finds out if there is presence of microscopic blood in stool.
Hemoglobin electrophoresis:
This test diagnoses sickle cell anemia or thalassemia.
Iron level:
Serum iron is ordered for figuring out either anemia is iron related or not. The normal range of iron in blood is 60 to 170 mcg/dL
Transferrin level or iron-binding capacity (TIBC)
Transferrin is a protein that binds iron in the blood. The normal range for transferrin is 170 to 370 mg/dl.
Ferritin:
Ferritin test helps to understand how much iron is storing in body.
Folate Test:
For diagnosing megaloblastic anemia Folate Test is advised.
Vitamin B12 Test:
Vitamin B-12 test is used to diagnose pernicious anemia.
Bilirubin:
Bilirubin is an enzyme produced from the breakdown of RBCs. The test is useful to diagnose hemolytic anemia.
Reticulocyte count:
Reticulocytes are immature red blood cells. The test is used to check erythropoiesis (formation of RBCs from bone marrow) and anemia.
Bone marrow biopsy, Liver function tests, Lead level and Kidney Function test are also important.
Erythrocytes normal values
Erythrocytes count
The normal RBC range for men is 4.7 to 6.1 million cells per microliter (mcL).
The normal RBC range for women/ female is 4.2 to 5.4 million cells per microliter (mcL).
PCV
Packed cell volume- the normal range of PCV is 0.40-0.55
MCV
The reference range for MCV (mean corpuscular volume) is 80-96 fL/red cell in adult.
MCH
The normal range for MCH (mean corpuscular hemoglobin, or mean cell hemoglobin) is between 27 and 33.2 picograms (pg).
MCHC
MCHC stands for mean corpuscular hemoglobin concentration its normal range is 30-35 g/100ml of red cell.